
Image courtesy of imagerymajestic / FreeDigitalPhotos.net
Health experts and breastfeeding experts agree that it’s best to wait until your baby is around six months old before offering any food other than breastmilk. There has been a large amount of research on this, and most health organizations have updated their recommendations to agree with current research. Unfortunately, many health care providers and written materials are not up to date in what they are advising parents.
Following are just a few of the organizations that recommend that all babies be exclusively breastfed (no cereal, juice or any other foods) for the first 6 months of life (not the first 4-6 months):
Now infants can get
all their vitamin D
from their mothers’ milk;
no drops needed with
our sponsor's
TheraNatal Lactation Complete
by THERALOGIX. Use PRC code “KELLY” for a special discount!
- World Health Organization
- UNICEF
- American Academy of Pediatrics
- American Academy of Family Physicians
- Australian National Health and Medical Research Council
- Health Canada
Most babies will become developmentally and physiologically ready to eat solid foods between 6 and 8 months of age.
Why wait until 6 months for solids?
Although many of the reasons listed here assume that your baby is breastfed or fed breastmilk only, experts generally recommend that solids be delayed for formula fed babies also.
- Baby will have greater protection from illness.
Although children continue to receive many immunities from breastmilk for as long as they breastfeed, the greatest immunity occurs while a baby is exclusively breastfed. Breastmilk contains 50+ known immune factors, and also facilitates the development of “good bacteria” that protect baby’s gut. Studies have shown that many illnesses and conditions are less likely to occur when baby receives any amount of breastmilk. Exclusive breastfeeding for at least 3-4 months (compared to non-exclusive breastfeeding) further decreases the risk of respiratory tract infections, ear infections, necrotizing enterocolitis (NEC), sudden infant death syndrome (SIDS), allergic disease, celiac disease, and type 1 diabetes. Exclusive breastfeeding for 6 months (compared to 4-6 months), further decreases the risk of gastrointestinal infection and respiratory infection. (AAP 2012, Naylor & Morrow 2001)
- Baby’s digestive system will have time to mature.
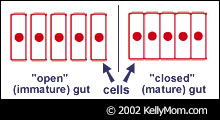 If solids are started before a baby’s system is ready to handle them, they are poorly digested and may cause unpleasant reactions (digestive upset, gas, constipation, etc.). Digestion of fats, protein, and complex carbohydrates is incomplete in infancy, but human milk contains enzymes that aid efficient digestion (Naylor & Morrow 2001).In addition, from birth until somewhere between four and six months of age babies possess what is often referred to as an “open gut.” This means that the spaces between the cells of the small intestines will readily allow intact macromolecules, including whole proteins and pathogens, to pass directly into the bloodstream. This is great for your breastfed baby as it allows beneficial antibodies in breastmilk to pass more directly into baby’s bloodstream, but it also means that large proteins from other foods (which may predispose baby to allergies) and disease-causing pathogens can pass right through, too. During baby’s first 4-6 months, while the gut is still “open,” antibodies (sIgA) from breastmilk coat baby’s digestive tract and provide passive immunity, reducing the likelihood of illness and allergic reactions before gut closure occurs. Baby starts producing these antibodies on his own at around 6 months, and gut closure should have occurred by this time also. For more on this subject, see: How Breast Milk Protects Newborns, and The Virgin Gut: A Note for Parents.
If solids are started before a baby’s system is ready to handle them, they are poorly digested and may cause unpleasant reactions (digestive upset, gas, constipation, etc.). Digestion of fats, protein, and complex carbohydrates is incomplete in infancy, but human milk contains enzymes that aid efficient digestion (Naylor & Morrow 2001).In addition, from birth until somewhere between four and six months of age babies possess what is often referred to as an “open gut.” This means that the spaces between the cells of the small intestines will readily allow intact macromolecules, including whole proteins and pathogens, to pass directly into the bloodstream. This is great for your breastfed baby as it allows beneficial antibodies in breastmilk to pass more directly into baby’s bloodstream, but it also means that large proteins from other foods (which may predispose baby to allergies) and disease-causing pathogens can pass right through, too. During baby’s first 4-6 months, while the gut is still “open,” antibodies (sIgA) from breastmilk coat baby’s digestive tract and provide passive immunity, reducing the likelihood of illness and allergic reactions before gut closure occurs. Baby starts producing these antibodies on his own at around 6 months, and gut closure should have occurred by this time also. For more on this subject, see: How Breast Milk Protects Newborns, and The Virgin Gut: A Note for Parents.
- Baby will be developmentally ready to eat foods that are not liquids.
A review done by Naylor & Morrow (2001) concluded, “These clinical reports indicate that the majority of normal full term infants are not developmentally ready for the transition from suckling to sucking or for managing semi-solids and solid foods in addition to liquids until between six and eight months of age.”
- Baby will have a lower risk of obesity in the future.
The early introduction of solids in infancy is associated with increased body fat and weight in adolescents and adults. (AAP 2012, Wilson 1998, von Kries 1999, Kalies 2005)
- Starting solids will be easier.
Babies who start solids later can feed themselves.
- Baby may have more protection from iron-deficiency anemia.
The introduction of iron supplements and iron-fortified foods, particularly during the first six months, reduces the efficiency of baby’s iron absorption. In one study of healthy, full-term infants (Pisacane, 1995), the researchers concluded that babies who were exclusively breastfed for 7 months (and were not give iron supplements or iron-fortified cereals) had significantly higher hemoglobin levels at one year than breastfed babies who received solid foods earlier than seven months. The researchers found no cases of anemia within the first year in babies breastfed exclusively for seven months and concluded that breastfeeding exclusively for seven months reduces the risk of anemia. See Is Iron-Supplementation Necessary? for more information.
- Mom will more easily maintain her milk supply.
Studies have shown that for babies under six months, solids tend to replace breastmilk in a baby’s diet – they do not add to baby’s total intake (WHO 2003, Cohen 1994, Dewey 1999). The more solids that baby eats, the less milk he takes from mom, and less milk taken from mom means less milk production. Babies who eat lots of solids or who start solids early tend to wean prematurely.
- Mom is less likely to become pregnant.
Breastfeeding is most effective in preventing pregnancy when your baby is exclusively breastfed and all of his nutritional and sucking needs are satisfied at the breast (Don’t believe this? It’s strongly supported by research – see Breastfeeding and Fertility for more information). Mothers who exclusively breastfeed for 6 months vs 4 months have a longer duration of lactational amenorrhea (the natural postpartum infertility that occurs when a woman is not menstruating due to breastfeeding). (Kramer & Kakuma, 2012)
- Mom can more quickly lose extra “baby weight.”
Mothers who exclusively breastfeed their babies for 6 months (compared to 4 months) have more rapid postpartum weight loss (Kramer & Kakuma, 2012).
Have you heard that foods should be introduced into the infant diet between 4 and 6 months to reduce the risk of developing allergy, celiac disease or type 1 diabetes mellitus?
The current evidence has been reviewed by several authorities, and the conclusion was that there is insufficient evidence to support the introduction of gluten (or other solid foods) into the infant diet before 6 months.
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD003517. DOI: 10.1002/14651858.CD003517.pub2.
“Although infants should still be managed individually so that insufficient growth or other adverse outcomes are not ignored and appropriate interventions are provided, the available evidence demonstrates no apparent risks in recommending, as a general policy, exclusive breastfeeding for the first six months of life in both developing and developed-country settings.” - American Academy of Pediatrics, Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics. 2012;129(3):e827-41.
“Overall, there is an association between increased duration of breastfeeding and reduced risk of celiac disease when measured as the presence of celiac antibodies. The critical protective factor appears to be not the timing of the gluten exposure but the overlap of breastfeeding at the time of the initial gluten ingestion. Thus, gluten-containing foods should be introduced while the infant is receiving only breast milk and not infant formula or other bovine milk products.” - SACN/COT statement on the timing of the introduction of gluten into the infant diet – March 2011.
SACN (Scientific Advisory Committee on Nutrition) and COT (Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment) in the UK concluded: “Overall currently available evidence on the timing of introduction of gluten into the infant diet and subsequent risk of coeliac disease and T1DM (type 1 diabetes mellitus) is insufficient to support recommendations about the appropriate timing of introduction of gluten into the infant diet beyond 3 completed months of age, for either the general population or high-risk sub-populations.” - WHO Statement: Exclusive breastfeeding for six months best for babies everywhere (15 January 2011)
- UNICEF UK response to media reports questioning the recommendation to introduce solid food to babies at 6 months (2011)
“Ensuring that the mother is not anaemic and that cord cutting is delayed will in turn ensure that the baby’s own body stores and breastmilk will provide sufficient iron for over 6 months. The majority of the food commonly introduced to babies in the early months such as cereal, fruit and vegetables are low in iron and will therefore not help prevent IDA. However, if they are introduced before a baby needs them, they will displace breastmilk from the baby’s diet and may thereby reduce the amount of iron consumed.””The incidence of genuine food allergy (as opposed to food intolerance) is rare. There is speculation and some observational data that when there is a family history of true allergy then early introduction of certain foods may be beneficial. Random control trials are now being undertaken to test this theory. Should this prove to be the case (which is by no means certain) then high risk families would need to be advised on a case-by-case basis. This would not affect public policy as applied to the majority of children not affected by allergies.” - Is baby’s risk for type I diabetes increased if solids are introduced before 3 months or after 6 months? at KellyMom
Additional information & references
- Solid Foods and the Breastfed Baby at KellyMom
- Is Iron-Supplementation Necessary? at KellyMom
- How can I tell if my baby is ready for solid foods? at KellyMom
- Will giving formula or solids at night help baby to sleep better? What about cereal in a bottle? at KellyMom
- Supplementation of the Breastfed Baby: “Just One Bottle Won’t Hurt”—or Will It? by Marsha Walker, RN, IBCLC
- How Breast Milk Protects Newborns by Jack Newman, MD
- Protective nutrients and bacterial colonization in the immature human gut (abstract)
- The Bacterial Flora of Humans by Kenneth Todar, PhD
“At birth the entire intestinal tract is sterile, but bacteria enter with the first feed. The initial colonizing bacteria vary with the food source of the infant. In breast-fed infants bifidobacteria account for more than 90% of the total intestinal bacteria. Enterobacteriaceae and enterococci are regularly present, but in low proportions, while bacteroides, staphylococci, lactobacilli and clostridia are practically absent. In bottle-fed infants, bifidobacteria are not predominant. When breast-fed infants are switched to a diet of cow’s milk or solid food, bifidobacteria are progressively joined by enterics, bacteroides, enterococci lactobacilli and clostridia. Apparently, human milk contains a growth factor that enriches for growth of bifidobacteria, and these bacteria play an important role in preventing colonization of the infant intestinal tract by non indigenous or pathogenic species.” - Breast-Milk: The White Blood by Arlene Jacobs
- WHO Resources on Child Nutrition
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD003517. DOI: 10.1002/14651858.CD003517.pub2.
- American Academy of Pediatrics, Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics. 2012;129(3):e827-41.
- WHO: Infant and young child feeding – Model Chapter for textbooks for medical students and allied health professionals (2009)
- Chantry CJ, Howard CR, Auinger P. Full breastfeeding duration and associated decrease in respiratory tract infection in US children. Pediatrics. 2006 Feb;117(2):425-32.
- WHO: Guiding Principles for feeding non-breastfed children 6-24 months of age (2005)
- WHO: Guiding principles for complementary feeding of the breastfed child (2003)
- WHO: Complementary feeding: report of the global consultation, and summary of guiding principles for complementary feeding of the breastfed child. (2002)
- WHO: The Optimal Duration of Exclusive Breastfeeding: A Systematic Review WHO/NHD/01.08 (2002)
- Optimal duration of exclusive breast feeding in low income countries (editorial). Black RE and Victora CG. BMJ 2002 (30 November);325:1252-1253.
 Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods: Reviews of the Relevant Literature Concerning Infant Gastrointestinal, Immunologic, Oral Motor and Maternal Reproductive and Lactational Development (April 2001), Audrey J. Naylor, MD, DrPH and Ardythe L Morrow, PhD, Editors.
Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods: Reviews of the Relevant Literature Concerning Infant Gastrointestinal, Immunologic, Oral Motor and Maternal Reproductive and Lactational Development (April 2001), Audrey J. Naylor, MD, DrPH and Ardythe L Morrow, PhD, Editors.- WHO: The Optimal Duration of Exclusive Breastfeeding: Report of an Expert Consultation WHO/FCH/CAH/01.24 (28-30 March 2001)
- Dewey KG, Cohen RJ, Brown KH, Rivera LL. Age of introduction of complementary foods and growth of term, low-birth-weight, breast-fed infants: a randomized intervention study in Honduras. Am J Clin Nutr. 1999;69(4):679-86.
- Sleisenger & Fordtran. Gastrointestinal and Liver Disease, 6th ed. W. B. Saunders Company (1998): p. 1495-1497.
- Rethinking current recommendations to introduce solid food between four and six months to exclusively breastfeeding infants. Borresen, HC. J Hum Lact 1995 Sep;11(3):201-4.
- Pisacane A, et al. Iron status in breast-fed infants. J Pediatr 1995 Sep;127(3):429-31.
- Cohen RJ, Brown KH, Canahuati J, Rivera LL, Dewey KG. Effects of age of introduction of complementary foods on infant breast milk intake, total energy intake, and growth: a randomised intervention study in Honduras. Lancet. 1994;344(8918):288-93.
Comparisons between different lengths of exclusive breastfeeding:
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD003517. DOI: 10.1002/14651858.CD003517.pub2.
- American Academy of Pediatrics, Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics. 2012;129(3):e827-41.
- SACN/COT statement on the timing of the introduction of gluten into the infant diet – March 2011.
- Kramer MS, Kakuma R. The optimal duration of exclusive breastfeeding: a systematic review. Adv Exp Med Biol. 2004;554:63-77.
From the abstract: Infants who are breastfed exclusively for 6 months experience less morbidity from gastrointestinal tract infection than infants who were mixed breastfed as of 3 or 4 months of age. No deficits have been demonstrated in growth among infants from either developing or developed countries who are exclusively breastfed for 6 months or longer. Moreover, the mothers of such infants have more prolonged lactational amenorrhea and faster postpartum weight loss. Based on the results of this review, the World Health Assembly adopted a resolution to recommend exclusive breastfeeding for 6 months to its member countries. - Onayade AA, Abiona TC, Abayomi IO, Makanjuola RO. The first six month growth and illness of exclusively and non-exclusively breast-fed infants in Nigeria. East Afr Med J. 2004 Mar;81(3):146-53.
CONCLUSION: It is concluded that exclusive breast-feeding supported adequate growth during the first six months of life for most of the infants studied. Early introduction of complementary foods did not provide any advantages in terms of weight gain in our environment, it was frequently associated with illness episodes and growth faltering. Many mothers however require support, encouragement and access to health care providers to breastfeed exclusively for the first six months of life. - Kramer MS, et al. Infant growth and health outcomes associated with 3 compared with 6 mo of exclusive breastfeeding. Am J Clin Nutr. 2003 Aug;78(2):291-5.
CONCLUSIONS: Exclusive breastfeeding for 6 mo is associated with a lower risk of gastrointestinal infection and no demonstrable adverse health effects in the first year of life. - WHO: The optimal duration of exclusive breastfeeding. A systematic review
WHO/FCH/CAH/01.23 (2002)
(compares introduction of solids at 3-4 months vs 6 months) - Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2002;(1):CD003517.
(compares introduction of solids at 3-4 months vs 6 months)
From the reviewer’s conclusions: “Infants who are exclusively breastfed for six months experience less morbidity from gastrointestinal infection than those who are mixed breastfed as of three or four months, and no deficits have been demonstrated in growth among infants from either developing or developed countries who are exclusively breastfed for six months or longer. Moreover, the mothers of such infants have more prolonged lactational amenorrhea.” - Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods: Reviews of the Relevant Literature Concerning Infant Gastrointestinal, Immunologic, Oral Motor and Maternal Reproductive and Lactational Development (April 2001), Audrey J. Naylor, MD, DrPH and Ardythe L Morrow, PhD, Editors.
- Dewey KG, Cohen RJ, Brown KH, Rivera LL. Effects of exclusive breastfeeding for four versus six months on maternal nutritional status and infant motor development: results of two randomized trials in Honduras. J Nutr. 2001 Feb;131(2):262-7.
- Hop LT, Gross R, Giay T, Sastroamidjojo S, Schultink W, Lang NT. Premature complementary feeding is associated with poorer growth of vietnamese children. J Nutr. 2000 Nov;130(11):2683-90.
(mainly compares introduction of solids before/after 3 mo) - Wilson AC, et al. Relation of infant diet to childhood health: seven year follow up of cohort of children in Dundee infant feeding study. BMJ 1998 January;316:21-25. (compares introduction of solids before/after 15 weeks)